ECG Hallucinations: When S1Q3T3 Misleads
Emergency Cardiology Literature Review & Updates with Dr. Amal Mattu
HPI
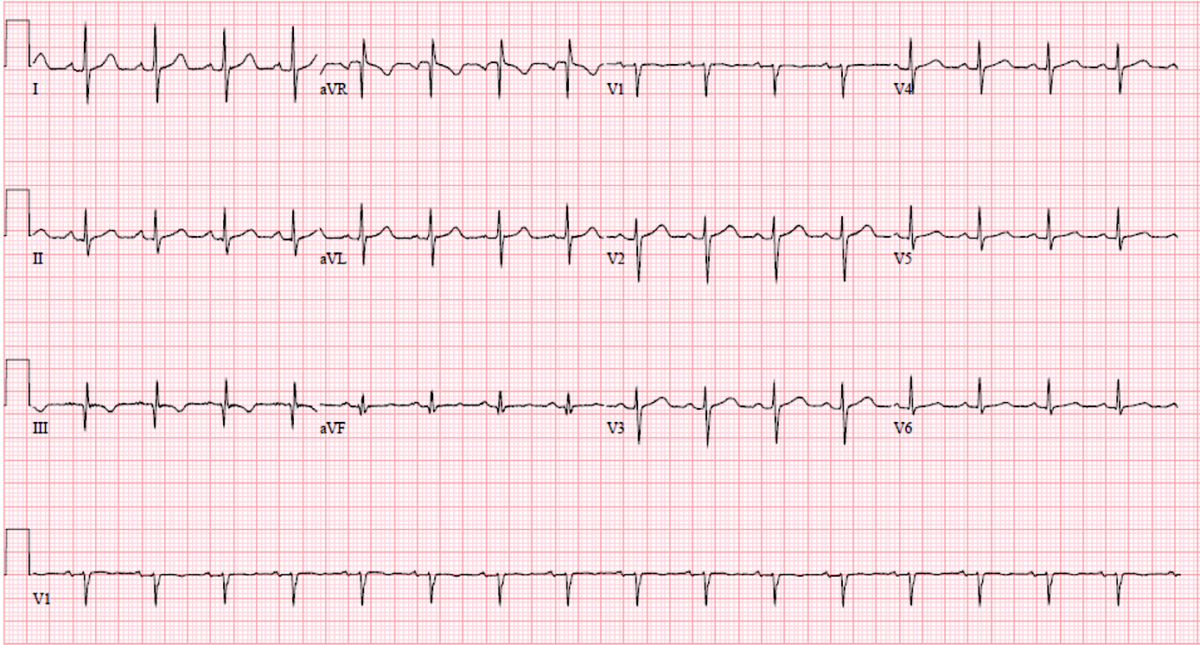
A 51-year-old truck driver presents to the ED after a brief syncopal episode at a rest stop. It is the middle of summer, his truck’s air conditioning is not working, he has had poor oral intake, and he appears clinically dehydrated. His vital signs are reassuring: afebrile, heart rate 100, respiratory rate 15, blood pressure 115/60, and fingerstick glucose 100. His exam is nondiagnostic except that he looks dehydrated. The following ECG is obtained and shows a pattern many clinicians are taught to associate with acute pulmonary embolism.
Before watching this week’s workout, review the ECG carefully and consider:
-
- Do you see an ECG pattern that has traditionally been associated with pulmonary embolism?
- When should an ECG finding meaningfully change your clinical probability enough to trigger additional testing?
- Which parts of “classic” ECG teaching are truly evidence-based, and which are repeated because they are memorable?
- In a syncope patient who clinically looks dehydrated, what ECG findings should actually make you worry about acute right heart strain or pulmonary embolism?
