Recent University of Maryland Medical Center Cases (Part III)
UMEM Potpourri ECG Cases with Dr. Amal Mattu
HPI
A 59-year-old man presents to the emergency department with chest pain and palpitations. The following ECG is obtained on arrival:
Before watching this week’s workout, carefully review the ECG and consider the following:
-
- What is your full rhythm interpretation?
- Does this rhythm typically need treatment with anticoagulation?
Video
Kudos
Thanks to the University of Maryland Medical Center's Department of Emergency Medicine for sharing their cases for this series.This episode is the last of a 3 part series of interesting recent cases from the University of Maryland Medical Center. This episode continues the discussion on AV blocks and bradydysrhythmias, emphasizing key diagnostic strategies, pitfalls, and pearls.
Case 10: Mobitz Type I AV Block (Wenckebach)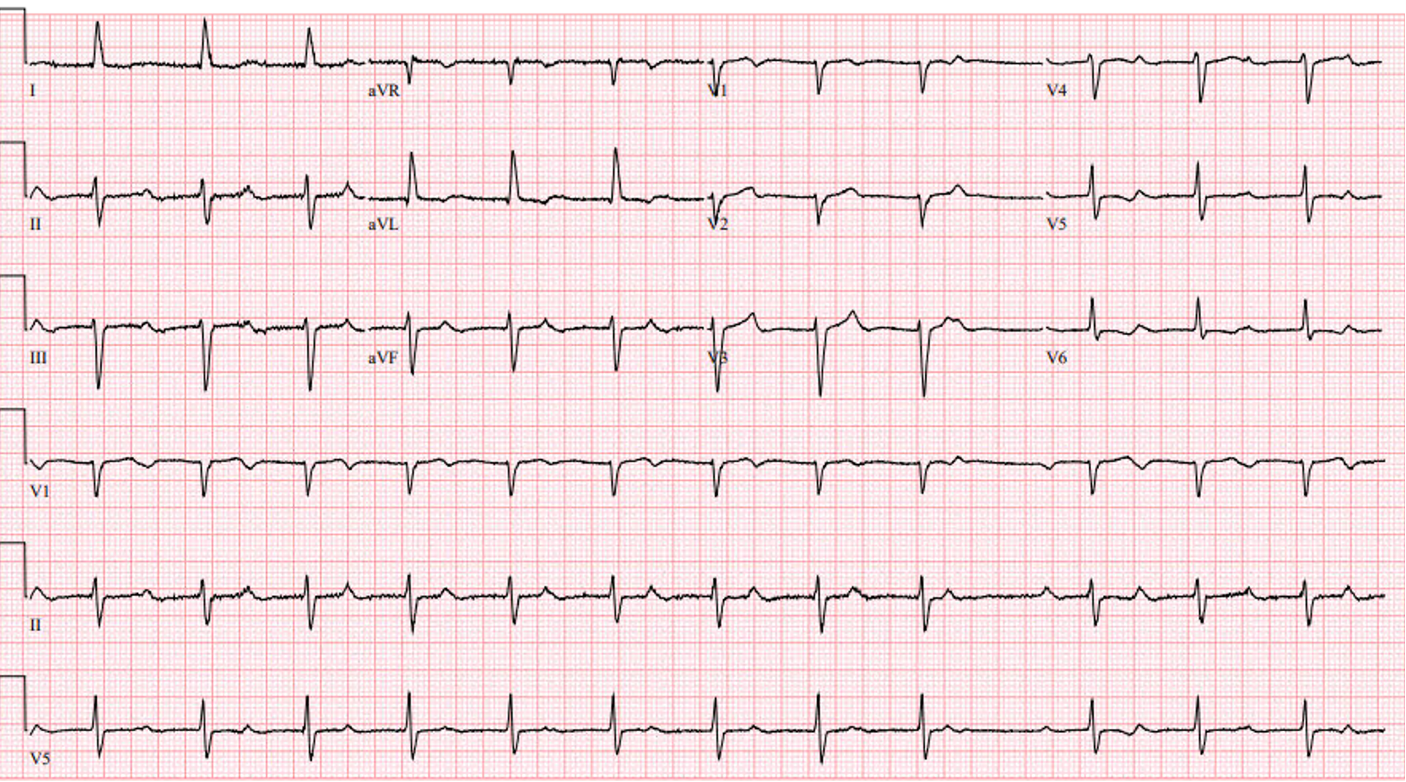
- Patient: 67-year-old woman with chest pain.
- Key ECG Finding:
- Slightly irregular rhythm with gradually lengthening PR intervals and periodic nonconducted (“lonely”) P waves.
- Hidden P waves within T waves (“pokey” T waves).
- Diagnosis: Slow-progressing Mobitz Type I (Wenckebach).
- Key Points:
- Mobitz I often shows progressively lengthening PR intervals until a dropped beat occurs.
- Always scrutinize suspicious T waves for hidden P waves (“electrocardiographic polyuria”).
Case 11: Complete Heart Block Mistaken for Mobitz II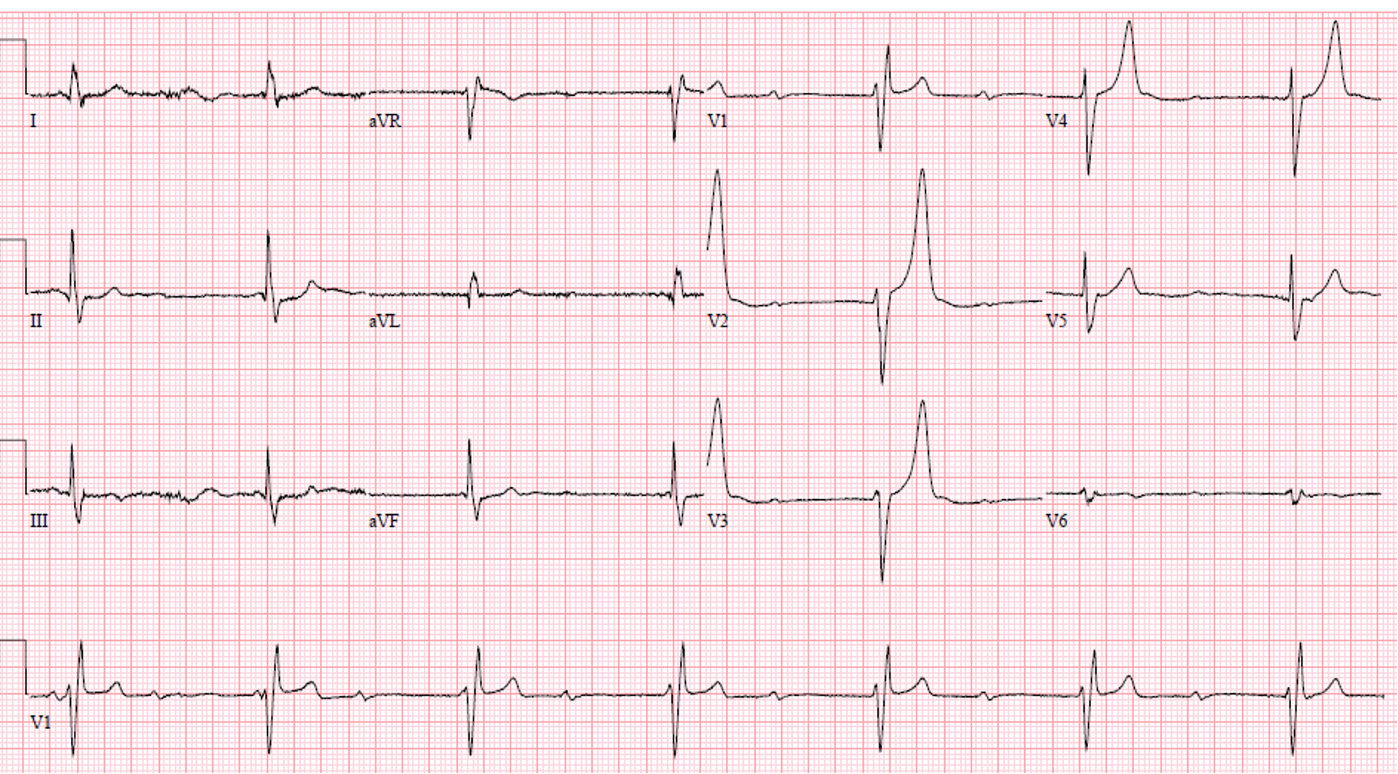
- Patient: 77-year-old man with lightheadedness.
- Key ECG Finding:
- Regular atrial rhythm with completely dissociated regular junctional escape rhythm (AV dissociation).
- Slight PR interval variability (not constant).
- Peaked T waves (potassium was normal)
- Diagnosis: Complete heart block with junctional escape rhythm and right bundle branch block pattern.
- Key Points:
- Mobitz II requires constant PR intervals; variability suggests complete heart block.
- Always confirm AV dissociation by carefully marching out P waves throughout all leads.
Case 12: Second-degree AV Block (2:1 Conduction)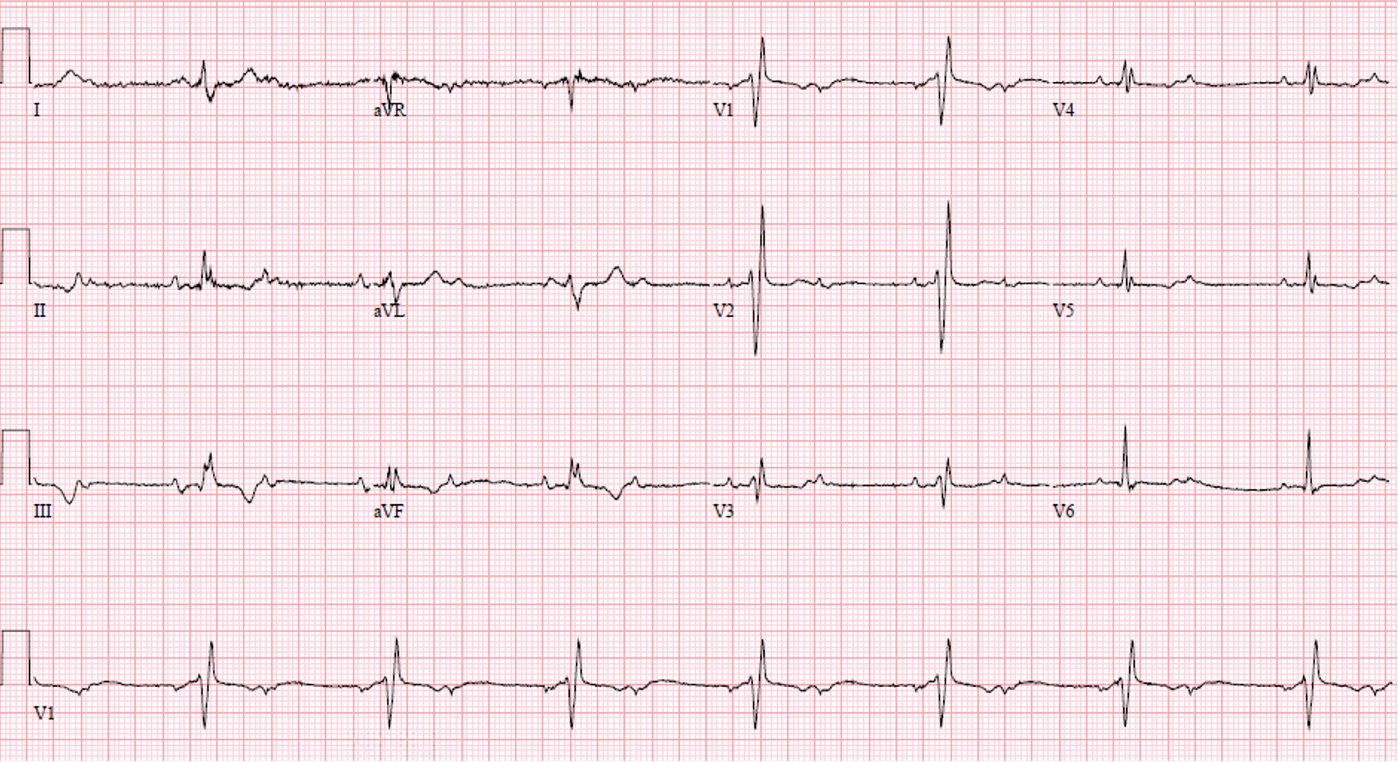
- Patient: 60-year-old woman with chest pain.
- Key ECG Findings:
- Regular rhythm with consistent 2:1 conduction (two P waves for each QRS complex).
- Narrow QRS complexes with right bundle branch block pattern.
- Diagnosis: Second-degree AV block with 2:1 conduction (cannot definitively distinguish Mobitz I vs. Mobitz II).
- Key Points:
- In 2:1 conduction, there’s insufficient PR interval information to distinguish Mobitz I from Mobitz II.
- This scenario produces a regular ventricular rhythm, the only instance when Mobitz rhythm is regular.
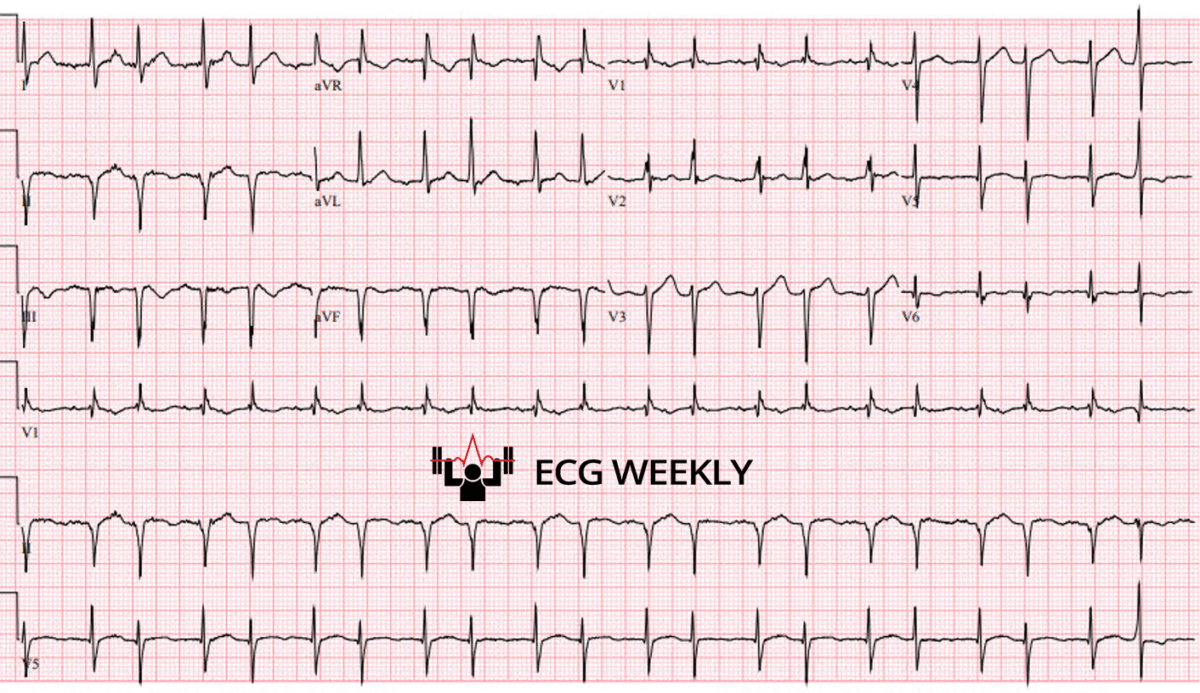
Case 13: Wenckebach Misdiagnosed as Atrial Fibrillation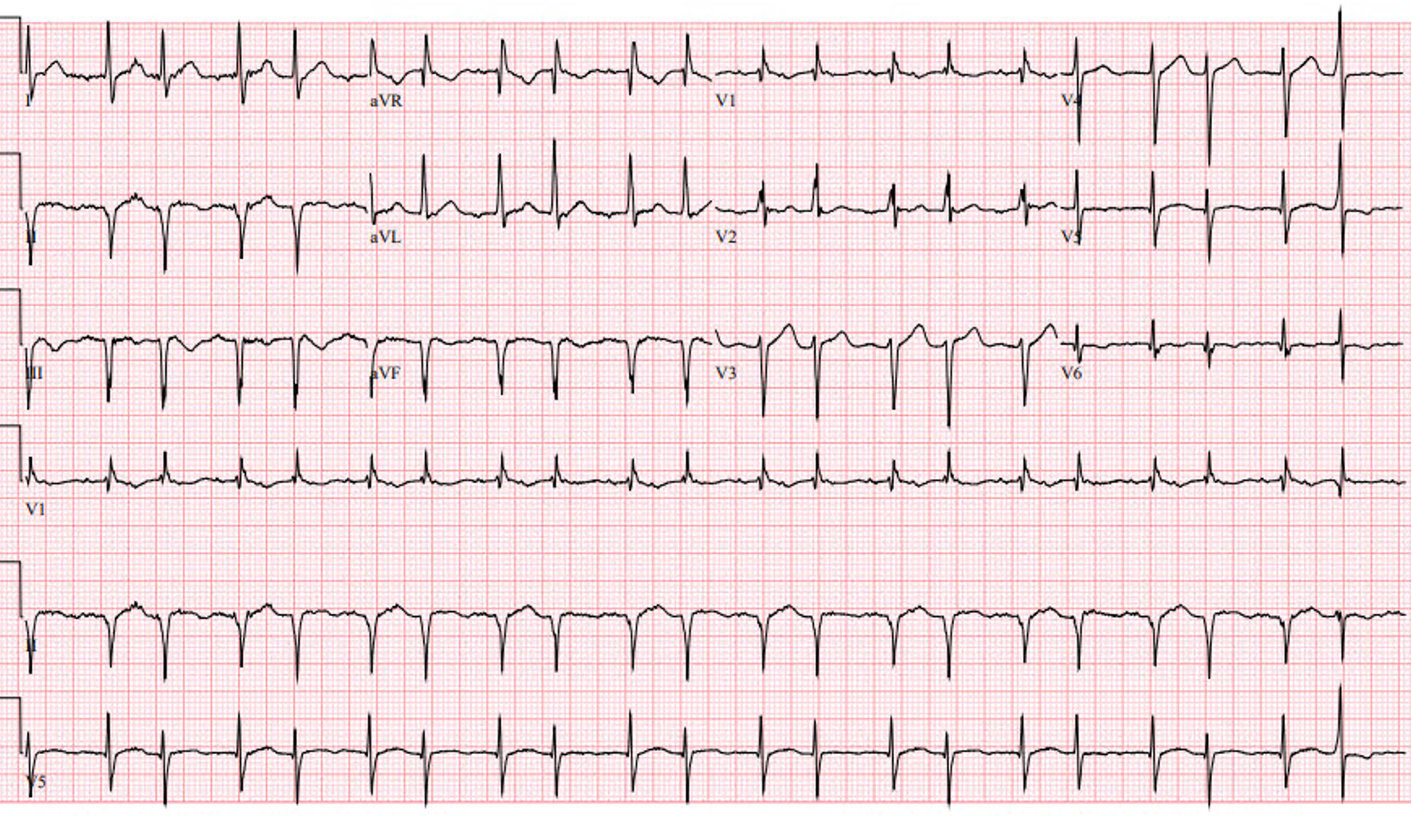
- Patient: 59-year-old man with chest pain.
- Key ECG Findings:
- Grouped beats (regularly irregular), initially misdiagnosed as atrial fibrillation.
- Progressive PR prolongation followed by dropped P waves (“lonely” P waves).
- Diagnosis: Mobitz Type I (Wenckebach) AV block with 3:2 conduction, incomplete right bundle branch block, prior inferior MI.
- Key Points:
- Grouped beats (“regularly irregular”) strongly suggest Mobitz or regularly occurring PACs, not atrial fibrillation (which is irregularly irregular).
- Confirm Mobitz by examining PR intervals and identifying nonconducted P waves.
Case 14: PACs Mimicking Mobitz AV Block (Atrial Bigeminy)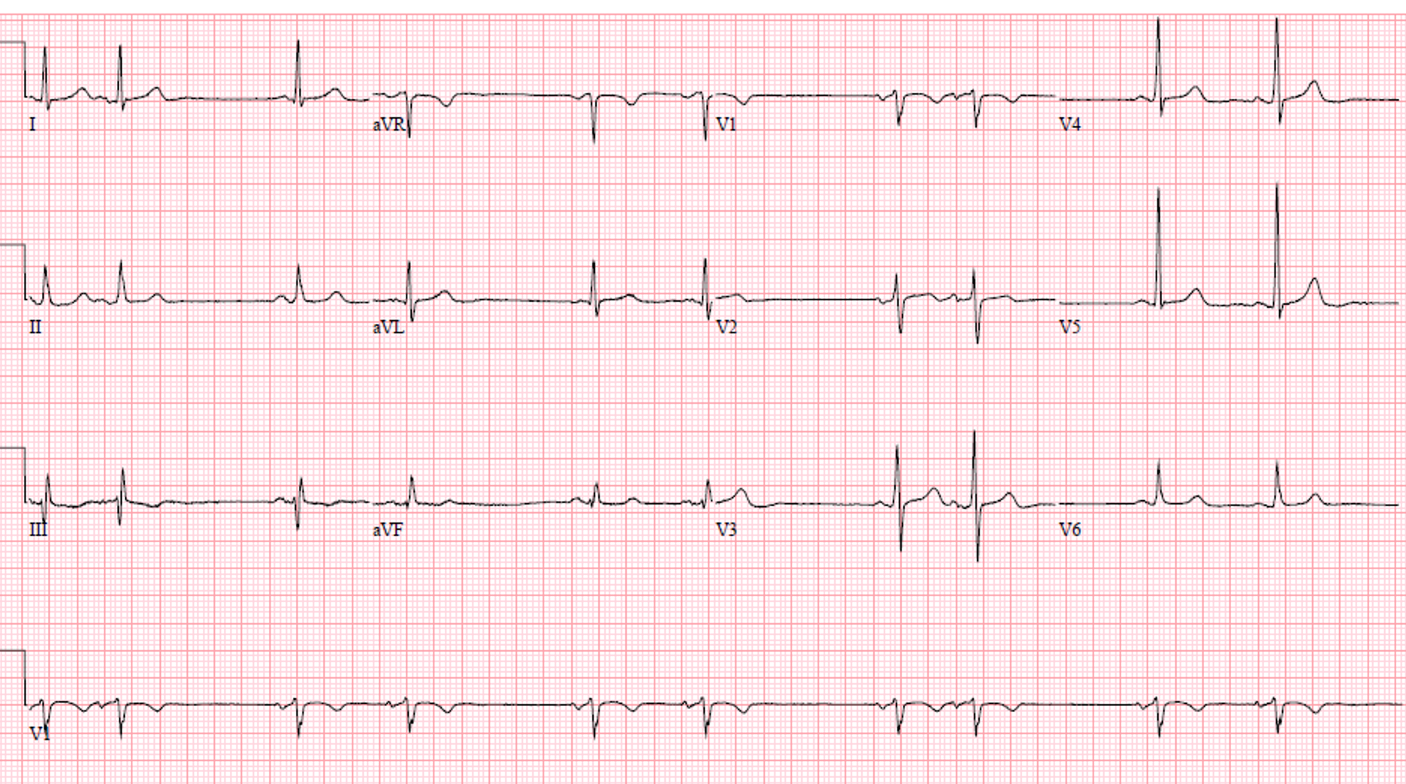
- Patient: 63-year-old man with palpitations.
- Key ECG Findings:
- Regularly irregular grouped beats (clumped beats).
- No evidence of lonely (nonconducted) P waves.
- PACs occurring every second beat, followed by a compensatory pause.
- Diagnosis: Sinus rhythm with atrial bigeminy (frequent PACs).
- Key Points:
- Regularly irregular rhythms suggest either Mobitz or PACs; differentiate by presence or absence of nonconducted P waves.
- PACs are a common cause of pauses and regularly occurring grouped beats.
Final Take Home Points:
- AV block differentiation: Always assess PR intervals carefully.
- Mobitz I (Wenckebach): Progressive PR prolongation before nonconducted P wave.
- Mobitz II: Constant PR intervals with occasional nonconducted P waves.
- Complete Heart Block: AV dissociation with regular escape rhythm; PR intervals vary.
- PACs vs. AV block: Grouped beats require close examination for lonely (nonconducted) P waves to differentiate Mobitz from PACs.
This week Dr. Mattu stressed systematic ECG analysis, careful caliper measurements, and skepticism toward automated ECG interpretations, ensuring accurate diagnosis and appropriate management. Next week we take a break from UMMC cases to review the 2025 ECG competition answers. Stay tuned!
