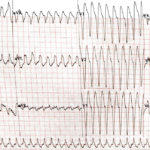
Wide QRS
Results:

Three High Risk ECGs and the Right Next Move
A 34 year old man presents with acute chest pain radiating to the left arm associated with diaphoresis. He has hyperlipidemia and a family history of early coronary disease. The…

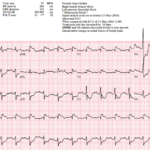
Occlusion MI in Left Bundle Branch Block (LBBB): STEMI Equivalent Pattern
Key Points: LBBB does not exclude acute coronary occlusion. LBBBs produce abnormal depolarization and expected secondary ST-T changes, which can mask or mimic ischemia. Acute occlusion MI can still be…
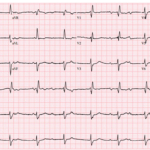
A Post-Arrest ECG With a Dangerous New Bundle Branch Block
A 72-year-old man is brought to the ED after a witnessed out-of-hospital cardiac arrest. Bystander CPR is started quickly, EMS finds a non-shockable rhythm, and ROSC is achieved after one…
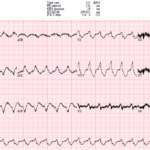
UMEM Cases, Part 4: When the Computer Misses the Rhythm and Flutter Fakes a STEMI
A 44-year-old man with severe cardiomyopathy, an LVAD, chronic amiodarone therapy, and an AICD presents with palpitations. His ECG shows a regular wide-complex tachycardia, but the rate is only 135….
Right Bundle Branch Block (RBBB)
Key Points: RBBB delays right ventricular activation. The left ventricle depolarizes normally through the left bundle, while the right ventricle is activated late by slow myocardial spread. ECG hallmark: QRS…
Left Bundle Branch Block (LBBB)
Key Points: LBBB delays left ventricular activation. The RV activates first through the intact right bundle, then the impulse spreads slowly from right to left across the septum and LV…
New RBBB + LAFB (Bifascicular Block) in ACS: OMI Pattern
Key Points: In a patient with ischemic symptoms, new RBBB + LAFB should raise concern for proximal LAD or septal ischemia until proven otherwise, especially if the patient has ongoing…
Wide QRS Complex: DDx
Key Points: A QRS duration greater than 120 ms reflects delayed or abnormal ventricular depolarization. A wide QRS may be chronic and benign in context, or it may be the…
Unstable Bradyarrhythmias
Key Points: Unstable bradyarrhythmias cause poor perfusion which can rapidly progress to shock, irreversible organ injury, or cardiac arrest. Priority: Do not treat the heart rate alone. Treat clinical instability….
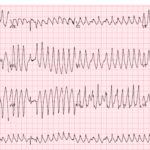
Polymorphic Ventricular Tachycardia (PMVT)
Key Points: Definition: Polymorphic ventricular tachycardia is VT with beat-to-beat variation in QRS morphology, axis, and amplitude. Clinical significance: PMVT is electrically unstable and can rapidly deteriorate into ventricular fibrillation…
Nonsustained Ventricular Tachycardia (NSVT)
Key Points: Definition: Nonsustained ventricular tachycardia is 3 or more consecutive ventricular beats lasting less than 30 seconds and terminating spontaneously. Rate: VT is usually faster than 120 bpm, but…
STEMI vs Wide QRS (BBBs & Paced Rhythms): DDx
Key Points: Wide QRS rhythms distort repolarization. Bundle branch block and ventricular pacing create secondary ST-T changes even without occlusion MI. Appropriate discordance is expected. ST segments and T waves…
Occlusion MI in Ventricular Paced Rhythms: STEMI Equivalent Pattern
Key Points: Ventricular paced rhythms can mask acute coronary occlusion. Pacing alters depolarization and produces expected secondary ST-T abnormalities, so standard STEMI criteria are unreliable. Appropriate discordance is expected in…
Ventricular Paced Rhythms
Key Points: Ventricular pacing changes depolarization and repolarization, so ST-T segments often look abnormal. In most paced rhythms, some discordant ST deviation is expected and should not be mistaken for…
Atrioventricular (AV) Block: Comprehensive Summary
Key Points: AV block refers specifically to delayed or failed conduction of impulses from the atria to the ventricles. AV block is classified by the ECG pattern of conduction: First-degree…
The Syncope ECG With Too Much P
A 68-year-old man has syncope, then has a second syncopal episode while lying still on a stretcher during evaluation at an outpatient clinic. He is sent emergently to the ED….
Left Ventricular Hypertrophy (LVH)
Key Points: LVH reflects increased left ventricular muscle mass, usually from chronic pressure overload. Common causes include longstanding hypertension and aortic stenosis. ECG diagnosis is imperfect. Voltage criteria are specific…

Preexcitation Pitfalls (Part 4): Potpourri Cases & Final Teaching Points
A 49-year-old man arrives with palpitations and chest discomfort. The monitor shows an irregular, wide-complex tachycardia with varying morphology and rates nearing 250 to 300 bpm. The team debates polymorphic…
Preexcitation Pitfalls (Part 3): Wide, Irregular, Fast…Avoid AV Nodal Blockers
A 53-year-old man presents with palpitations and lightheadedness. The following ECG is obtained on arrival and appears very rapid and irregular with changing QRS morphologies. He starts showing signs of…
Preexcitation Pitfalls (Part 2): Wide, Regular, Fast…Treat It Like VT
A young man with recurrent palpitations presents to the emergency department hemodynamically stable during an episode. The arrival ECG shows a wide complex, regular tachycardia and the computer interpretation calls…
ECG Tags
- A-Z
- ACS Mimics
- ACS-OMI
- Activation
- Advanced Level Curriculum
- Annual ECG Competition
- Anterior OMI
- Anterior STEMI
- Approach
- Arrest
- Arrhythmia
- Arrhythmogenic Cardiomyopathy
- Artifact
- ARVC
- ARVD
- Atrial Parasystole
- Attending
- AV Block
- aVF
- aVL
- aVR
- Axis
- Barcelona
- Basics
- Bix Rule
- Board Review
- Bradyarrhythmia
- Cath Lab
- Chest Pain
- Clumped Beats
- Competition
- Conduction
- Core
- Core Level Curriculum
- Critical ECG Patterns
- Curriculum
- DDx
- Delta
- Devices
- Diagonal Branch Occlusion
- Differential Diagnoses
- Diffuse ST Elevation
- Documentation
- Early Repolarization
- ECG Interpretation
- ECG Localization
- ECG Variant
- Education/Teaching
- Electrolytes
- Emergencies
- Emergent Cath Lab Activation
- EMS
- Expert Level Curriculum
- Flutter
- Flutter Waves
- Foundations Level Curriculum
- Guidelines
- High-Lateral STEMI
- Hub
- Hyperacute T waves
- Hypercalcemia
- Hyperkalemia
- Hypermagnesemia
- Hypocalcemia
- Hypokalemia
- Hypomagnesemia
- Hyponatremia
- Hypothermia
- I
- II
- Index
- Inferior OMI
- Inferior STEMI
- Intervals
- Irregular
- Ischemia
- Ischemia & Infarction
- J point
- J Waves
- JT
- Junctional Rhythm
- Juvenile T wave
- LAD Occlusion
- Lateral STEMI
- LBBB
- LCx Occlusion
- Lead Placement
- Left Atrial Enlargement (LAE)
- Life Savers
- LV an
- LV Aneurysm
- LVAD
- Mastery Level Curriculum
- Metabolic
- Mimics
- Morphology
- Narrow QRS
- Occlusion MI
- OMI Pattern
- Orthodromic AVRT
- Osborn Waves
- P Wave
- Paced Rhythms
- Pacemaker/ICD
- Paramedics
- Pauses
- PE
- Pediatrics
- Pericardial
- Pericarditis
- PGY-1
- PGY-2
- PGY-3
- PGY-4
- Post-Arrest
- post-arrest STEMI
- Post-Cardiac Arrest
- Posterior Extension
- Posterior MI
- Posterior STEMI
- potpourri
- PR
- Preexcitation
- Premature Complexes
- Prolonged QT
- Pulmonary Embolism
- Pulse-Tapping Artifact
- PVCs
- Q Wave
- QRS
- QT
- R Waves
- RAD
- Rate
- RBBB
- RCA Occlusion
- Regular
- Reperfusion
- Rhythm
- Right Atrial Enlargement (RAE)
- RR
- S Waves
- S1Q3T3
- Segments
- Seizure
- Serial ECGs
- Sgarbossa
- Shock
- South African Flag Sign
- ST
- ST Depression
- ST Elevation
- STEMI
- STEMI Equivalent
- STEMI Mimics
- STEMI Negative OMI
- Stepwise
- Stroke
- Structural
- Students
- SVT
- Syncope
- T Wave Inversion
- T Waves
- Tachyarrhythmia
- Tachycardia
- Tamponade
- Terminal QRS Distortion
- Toxicology
- TP
- Traditional STEMI Criteria
- U Waves
- Unstable
- V1-V4
- V2
- V5
- V6
- Vectors
- Ventricular Repolarization
- Ventricular Rhythms
- Ventricular Tachycardia
- Voltage
- Waveforms
- Wide QRS
- Workflow
- WPW
© 2026 ECG Weekly. All rights reserved. | Terms of Use | Privacy Policy
Powered by the member(dev) platform
 Loading...
Loading...