Bradyarrhythmia
Results:
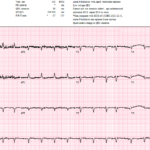
The Rhythm Behind the Irregularity
A 69-year-old woman presenting with sepsis gets the following ECG for tachycardia while febrile and shivering. The baseline is poor, atrial activity is difficult to identify, and the computer interpretation…

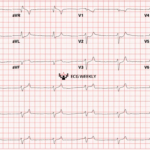
Three High Risk ECGs and the Right Next Move
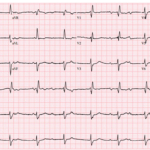
A 34 year old man presents with acute chest pain radiating to the left arm associated with diaphoresis. He has hyperlipidemia and a family history of early coronary disease. The…
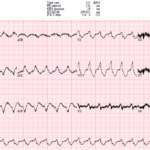
The Cath Lab Was Activated, But Something Didn’t Fit
A 70-year-old woman with CHF, COPD, intermittent atrial fibrillation, chronic pain medication use, and recent poor intake develops sudden dyspnea at rest and is found somnolent and bradycardic in the…

Sinus Node Dysfunction (Sick Sinus Syndrome & Bradycardia-Tachycardia Syndrome)
Key Points: A spectrum, not a single rhythm: Sinus node dysfunction includes inappropriate sinus bradycardia, sinus pauses or arrest, SA exit block, chronotropic incompetence, and alternating atrial tachyarrhythmias with bradycardia….
UMEM Cases, Part 4: When the Computer Misses the Rhythm and Flutter Fakes a STEMI
A 44-year-old man with severe cardiomyopathy, an LVAD, chronic amiodarone therapy, and an AICD presents with palpitations. His ECG shows a regular wide-complex tachycardia, but the rate is only 135….
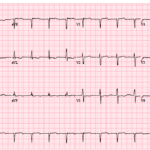
UMEM Cases, Part 3: When the Diagnosis Seems Clear and When It Is Not
A 71-year-old man presents with shortness of breath, and his ECG is initially read as a junctional rhythm. On later review, it is even mistaken for atrial fibrillation. But the…
Unstable Bradyarrhythmias
Key Points: Unstable bradyarrhythmias cause poor perfusion which can rapidly progress to shock, irreversible organ injury, or cardiac arrest. Priority: Do not treat the heart rate alone. Treat clinical instability….
Junctional Rhythms
Key Points: Junctional rhythms arise from the AV junction, usually the AV node or proximal His bundle, when the sinus node slows, fails, or impulses do not reach the ventricles…
The Syncope ECG With Too Much P
A 68-year-old man has syncope, then has a second syncopal episode while lying still on a stretcher during evaluation at an outpatient clinic. He is sent emergently to the ED….
Third-Degree AV Block (Complete Heart Block)
Key Points: Third-degree AV block is complete failure of atrial impulses to conduct to the ventricles. The defining ECG feature is AV dissociation with no conducted P waves. The atrial…
Second-Degree AV Block Type I (Mobitz I/Wenckebach)
Key Points: Mobitz I is defined by progressive PR prolongation until a single P wave fails to conduct, after which the cycle resets. The block is usually at the AV…
Second-Degree AV Block with 2:1 Conduction
Key Points: Second-degree AV block with 2:1 conduction means every other P wave conducts and every other P wave is blocked. A single ECG with 2:1 conduction usually cannot be…
First-Degree AV Block
Key Points: First-degree AV block is defined by a PR interval greater than 200 ms with fixed 1:1 AV conduction and no dropped QRS complexes. It usually reflects delayed conduction,…
Second-Degree AV Block Type II (Mobitz II)
Key Points: Mobitz II is defined by sudden failure of AV conduction after at least 2 consecutive conducted beats with fixed PR intervals and no preceding PR prolongation. The block…
Advanced (High-Grade) AV Block
Key Points: Advanced or high-grade AV block is a severe second-degree AV block with 2 or more consecutive non-conducted P waves, such as 3:1 or 4:1 conduction. Do not force…
BRASH Syndrome
Key Points BRASH is a synergistic spiral: bradycardia, renal failure, therapeutic AV-nodal blockade, shock, and hyperkalemia. The signature clue is disproportionate brady-shock despite only modest potassium elevation. Do not be…
Narrow QRS Bradycardia: DDx
Key Point Narrow QRS bradycardias are often related to vagal tone or reversible causes, but not always benign. Certain AV blocks and conduction abnormalities may still carry significant risk, even…
Ventricular Escape Rhythms
Key Points Wide QRS Complex Rhythm: Ventricular escape rhythms (aka idioventricular rhythms) are characterized by a wide QRS duration (>120 ms), absent or dissociated P-waves, and a regular, slow ventricular…
Sinus Bradycardia
Key Points: Definition: Sinus bradycardia is a rhythm originating from the sinoatrial (SA) node with a rate < 60 bpm. Physiological Occurrence: Common in young, healthy adults, athletes, and during…
Bradycardia: DDx
Key Points Common Offenders: Beta-blockers, calcium channel blockers, and digoxin often top the list of medication-induced bradycardia. High Vagal Tone or AV Block can arise from structural heart disease, ischemia,…
ECG Tags
- A-Z
- ACS Mimics
- ACS-OMI
- Activation
- Advanced Level Curriculum
- Annual ECG Competition
- Anterior OMI
- Anterior STEMI
- Approach
- Arrest
- Arrhythmia
- Arrhythmogenic Cardiomyopathy
- Artifact
- ARVC
- ARVD
- Atrial Parasystole
- Attending
- AV Block
- aVF
- aVL
- aVR
- Axis
- Barcelona
- Basics
- Bix Rule
- Board Review
- Bradyarrhythmia
- Cath Lab
- Chest Pain
- Clumped Beats
- Competition
- Conduction
- Core
- Core Level Curriculum
- Critical ECG Patterns
- Curriculum
- DDx
- Delta
- Devices
- Diagonal Branch Occlusion
- Differential Diagnoses
- Diffuse ST Elevation
- Documentation
- Early Repolarization
- ECG Interpretation
- ECG Localization
- ECG Variant
- Education/Teaching
- Electrolytes
- Emergencies
- Emergent Cath Lab Activation
- EMS
- Expert Level Curriculum
- Flutter
- Flutter Waves
- Foundations Level Curriculum
- Guidelines
- High-Lateral STEMI
- Hub
- Hyperacute T waves
- Hypercalcemia
- Hyperkalemia
- Hypermagnesemia
- Hypocalcemia
- Hypokalemia
- Hypomagnesemia
- Hyponatremia
- Hypothermia
- I
- II
- Index
- Inferior OMI
- Inferior STEMI
- Intervals
- Irregular
- Ischemia
- Ischemia & Infarction
- J point
- J Waves
- JT
- Junctional Rhythm
- Juvenile T wave
- LAD Occlusion
- Lateral STEMI
- LBBB
- LCx Occlusion
- Lead Placement
- Left Atrial Enlargement (LAE)
- Life Savers
- LV an
- LV Aneurysm
- LVAD
- Mastery Level Curriculum
- Metabolic
- Mimics
- Morphology
- Narrow QRS
- Occlusion MI
- OMI Pattern
- Orthodromic AVRT
- Osborn Waves
- P Wave
- Paced Rhythms
- Pacemaker/ICD
- Paramedics
- Pauses
- PE
- Pediatrics
- Pericardial
- Pericarditis
- PGY-1
- PGY-2
- PGY-3
- PGY-4
- Post-Arrest
- post-arrest STEMI
- Post-Cardiac Arrest
- Posterior Extension
- Posterior MI
- Posterior STEMI
- potpourri
- PR
- Preexcitation
- Premature Complexes
- Prolonged QT
- Pulmonary Embolism
- Pulse-Tapping Artifact
- PVCs
- Q Wave
- QRS
- QT
- R Waves
- RAD
- Rate
- RBBB
- RCA Occlusion
- Regular
- Reperfusion
- Rhythm
- Right Atrial Enlargement (RAE)
- RR
- S Waves
- S1Q3T3
- Segments
- Seizure
- Serial ECGs
- Sgarbossa
- Shock
- South African Flag Sign
- ST
- ST Depression
- ST Elevation
- STEMI
- STEMI Equivalent
- STEMI Mimics
- STEMI Negative OMI
- Stepwise
- Stroke
- Structural
- Students
- SVT
- Syncope
- T Wave Inversion
- T Waves
- Tachyarrhythmia
- Tachycardia
- Tamponade
- Terminal QRS Distortion
- Toxicology
- TP
- Traditional STEMI Criteria
- U Waves
- Unstable
- V1-V4
- V2
- V5
- V6
- Vectors
- Ventricular Repolarization
- Ventricular Rhythms
- Ventricular Tachycardia
- Voltage
- Waveforms
- Wide QRS
- Workflow
- WPW
© 2026 ECG Weekly. All rights reserved. | Terms of Use | Privacy Policy
Powered by the member(dev) platform
 Loading...
Loading...