Core
Results:
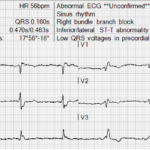
UMMC Cases Part II: Grouped Beats, Slow VT, and Diffuse ST Elevation
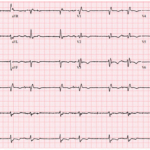
A 63-year-old man presents with shortness of breath. His ECG shows an unusual rhythm with repetitive groups of two beats separated by pauses.

Inverted P Waves in V1: DDx
Key Points: Know What Is Normal: The sinus P wave in V1 is often biphasic, with an initial positive and terminal negative component. A predominantly or completely negative P wave…
Slow Ventricular Tachycardia (VT)
Key Points: Definition: Slow VT refers to ventricular tachycardia occurring at an unusually low ventricular rate, often near or even below the conventional tachycardia threshold. There is no universally accepted…
Ventricular Tachycardia (VT) Mimics
Key Points: Default assumption: A regular wide-complex tachycardia should be considered VT until another diagnosis is more likely. Rate modifies the differential, not the diagnosis. Typical monomorphic VT is often…
ECG Hallucinations: When Irregular Is Not Atrial Fibrillation
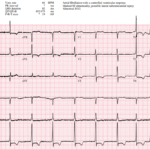
A 69-year-old man presents with chest pain. His ECG is interpreted by the computer as atrial fibrillation, a diagnosis that could significantly alter his evaluation and long-term management. The rhythm…
ECG Hallucinations: When S1Q3T3 Misleads
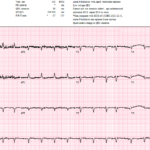
A 51-year-old truck driver presents to the ED after a brief syncopal episode at a rest stop. It is the middle of summer, his truck’s air conditioning is not working,…
ST Depression V1-V4: OMI Pattern
Key Points: Posterior OMI can hide on the standard 12-lead. Acute posterior coronary occlusion may produce no diagnostic ST elevation in the conventional leads. Instead, posterior ST elevation is seen…
S1Q3T3 Pattern
Key Points: Not a PE diagnosis: S1Q3T3 is classically associated with pulmonary embolism, but it is neither sensitive nor specific enough to diagnose or exclude PE. Think acute right heart…
ECG in Pulmonary Embolism (PE)
Key Points: The ECG cannot rule in or rule out PE: No single ECG finding is sufficiently sensitive or specific to diagnose or exclude acute pulmonary embolism. A Normal ECG…
High Risk Pulmonary Embolism (PE)
Key Points: The ECG can provide an early warning of severe RV strain: No ECG finding defines high risk PE, but marked or evolving signs of acute RV pressure overload…
The Rhythm Behind the Irregularity
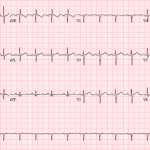
A 69-year-old woman presenting with sepsis gets the following ECG for tachycardia while febrile and shivering. The baseline is poor, atrial activity is difficult to identify, and the computer interpretation…
STEMI vs Early Repolarization: DDx
Key Points: Early repolarization (ER) is one of the most common non-ischemic causes of ST elevation and one of the most frequent ECG mimics of acute anterior coronary occlusion. The…
A Closer Look at the J Point
A 72-year-old man undergoes a prehospital 12-lead ECG. The tracing appears to show ST segment elevation in leads III, aVF, and aVR, raising concern for an inferior STEMI or high-risk…

Three High Risk ECGs and the Right Next Move
A 34 year old man presents with acute chest pain radiating to the left arm associated with diaphoresis. He has hyperlipidemia and a family history of early coronary disease. The…
Understanding ECG Artifacts
Key Points: Definition: ECG artifact is a noncardiac signal that distorts, obscures, or mimics the heart’s true electrical activity. Common sources: Patient movement or muscle activity, poor electrode contact, lead…
Barcelona Criteria in Left Bundle Branch Block (LBBB): OMI Pattern
Key Points: The Barcelona Criteria are ECG criteria proposed to identify acute myocardial infarction in patients with LBBB. Core problem: LBBB causes expected secondary ST-T changes, so standard STEMI millimeter…
Aslanger Pattern: OMI Pattern
Key Points: Aslanger pattern is an OMI pattern that can identify acute inferior occlusion despite not meeting traditional STEMI criteria. The key finding is ST segment elevation isolated to lead…
Occlusion MI in Left Bundle Branch Block (LBBB): STEMI Equivalent Pattern
Key Points: LBBB does not exclude acute coronary occlusion. LBBBs produce abnormal depolarization and expected secondary ST-T changes, which can mask or mimic ischemia. Acute occlusion MI can still be…
Sinus Bradycardia
Key Points: Definition: Sinus bradycardia is a sinus rhythm with a rate <60 bpm. In clinical practice, a rate <50 bpm is often a more useful threshold because resting rates…
J Point: Basics
Key Points: The J point is the junction between the end of the QRS complex and the beginning of the ST segment. It is a location, not a separate waveform….
ECG Tags
- A-Z
- ACS Mimics
- ACS-OMI
- Activation
- Advanced Level Curriculum
- Annual ECG Competition
- Anterior OMI
- Anterior STEMI
- Approach
- Arrest
- Arrhythmia
- Arrhythmogenic Cardiomyopathy
- Artifact
- ARVC
- ARVD
- Atrial Parasystole
- Attending
- AV Block
- aVF
- aVL
- aVR
- Axis
- Barcelona
- Basics
- Bix Rule
- Board Review
- Bradyarrhythmia
- Cath Lab
- Chest Pain
- Clumped Beats
- Competition
- Conduction
- Core
- Core Level Curriculum
- Critical ECG Patterns
- Curriculum
- DDx
- Delta
- Devices
- Diagonal Branch Occlusion
- Differential Diagnoses
- Diffuse ST Elevation
- Documentation
- Early Repolarization
- ECG Interpretation
- ECG Localization
- ECG Variant
- Education/Teaching
- Electrolytes
- Emergencies
- Emergent Cath Lab Activation
- EMS
- Expert Level Curriculum
- Flutter
- Flutter Waves
- Foundations Level Curriculum
- Guidelines
- High-Lateral STEMI
- Hub
- Hyperacute T waves
- Hypercalcemia
- Hyperkalemia
- Hypermagnesemia
- Hypocalcemia
- Hypokalemia
- Hypomagnesemia
- Hyponatremia
- Hypothermia
- I
- II
- Index
- Inferior OMI
- Inferior STEMI
- Intervals
- Irregular
- Ischemia
- Ischemia & Infarction
- J point
- J Waves
- JT
- Junctional Rhythm
- Juvenile T wave
- LAD Occlusion
- Lateral STEMI
- LBBB
- LCx Occlusion
- Lead Placement
- Left Atrial Enlargement (LAE)
- Life Savers
- LV an
- LV Aneurysm
- LVAD
- Mastery Level Curriculum
- Metabolic
- Mimics
- Morphology
- Narrow QRS
- Occlusion MI
- OMI Pattern
- Orthodromic AVRT
- Osborn Waves
- P Wave
- Paced Rhythms
- Pacemaker/ICD
- Paramedics
- Pauses
- PE
- Pediatrics
- Pericardial
- Pericarditis
- PGY-1
- PGY-2
- PGY-3
- PGY-4
- Post-Arrest
- post-arrest STEMI
- Post-Cardiac Arrest
- Posterior Extension
- Posterior MI
- Posterior STEMI
- potpourri
- PR
- Preexcitation
- Premature Complexes
- Prolonged QT
- Pulmonary Embolism
- Pulse-Tapping Artifact
- PVCs
- Q Wave
- QRS
- QT
- R Waves
- RAD
- Rate
- RBBB
- RCA Occlusion
- Regular
- Reperfusion
- Rhythm
- Right Atrial Enlargement (RAE)
- RR
- S Waves
- S1Q3T3
- Segments
- Seizure
- Serial ECGs
- Sgarbossa
- Shock
- South African Flag Sign
- ST
- ST Depression
- ST Elevation
- STEMI
- STEMI Equivalent
- STEMI Mimics
- STEMI Negative OMI
- Stepwise
- Stroke
- Structural
- Students
- SVT
- Syncope
- T Wave Inversion
- T Waves
- Tachyarrhythmia
- Tachycardia
- Tamponade
- Terminal QRS Distortion
- Toxicology
- TP
- Traditional STEMI Criteria
- U Waves
- Unstable
- V1-V4
- V2
- V5
- V6
- Vectors
- Ventricular Repolarization
- Ventricular Rhythms
- Ventricular Tachycardia
- Voltage
- Waveforms
- Wide QRS
- Workflow
- WPW
© 2026 ECG Weekly. All rights reserved. | Terms of Use | Privacy Policy
Powered by the member(dev) platform
 Loading...
Loading...