ACS-OMI
Results:

Modified Sgarbossa Criteria: STEMI Equivalent Pattern
Key Points: LBBB and ventricular-paced rhythms can hide acute coronary occlusion because abnormal depolarization creates expected secondary ST-T changes. Occlusion MI can still be recognized when those ST changes are…
Appropriate Discordance
Key Points: Appropriate discordance refers to the expected secondary ST segment and T wave pattern seen with abnormal ventricular depolarization, especially LBBB and ventricular-paced rhythm. The ST segment and T…
ST Depression: DDx
Key Points: ST depression is a pattern, not a diagnosis. It can represent ischemia, reciprocal change, baseline repolarization abnormalities, or noncardiac physiology. First split: regional (territorial) ST depression vs diffuse…
WPW Syndrome and Pseudo-MI Patterns
Key Points: WPW alters ventricular depolarization, producing secondary repolarization abnormalities that can mimic or mask myocardial infarction. ST-segment deviation in WPW is often non-ischemic, driven by abnormal activation via the…
Baltimore City EMS ECGs: Pitfalls and Mimics (Part 1)
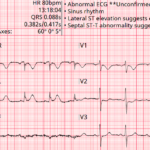
A 68-year-old man is brought to the emergency department by EMS with acute chest discomfort. The following prehospital ECG was obtained and shows concave ST elevation across multiple leads. The…
Four ECG Pitfalls That Punish Anchoring Bias
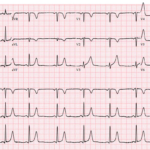
A 43-year-old woman with sharp left-sided chest pain and minimal cardiac risk factors has an initial ECG that is not diagnostic for STEMI. She looks stable, but one feature on…
Occlusion MI: STEMI Criteria & Beyond
Key Points: The ECG’s primary role in ACS is detecting acute coronary occlusion. Acute coronary occlusion myocardial infarction (OMI) is a time-critical diagnosis that requires immediate reperfusion. Time is myocardium….
STEMI (-) Occlusion MI: OMI Patterns
Key Points: Traditional STEMI criteria miss many acute coronary occlusions. A substantial proportion of true OMIs do not meet classic millimetric STEMI thresholds. OMI is a pathophysiologic diagnosis, not an…
STEMI in the Presence of Baseline ECG Abnormalities
Key Points: Baseline ECG abnormalities do not protect patients from occlusion MI. They increase miss rates because they distort the ST segment and T waves. The core question is not…
Lateral and High-Lateral STEMI: Criteria, Localization, and Pitfalls
Key Points: Lateral and high-lateral STEMI often present with subtle ST elevation and are commonly missed or labeled as nonspecific ST-T changes. Small-appearing ECG changes may represent true coronary occlusion…
Inferior STEMI: Criteria, RV Involvement, and Pitfalls
Key Points: Inferior STEMI is the most common STEMI subtype and is frequently complicated by right ventricular and posterior involvement. Inferior occlusion may present with classic ST elevation, subtle ischemic…
Anterior STEMI: Criteria, Localization, and Pitfalls
Key Points: Anterior STEMI represents large myocardial territory at risk and carries the highest mortality among STEMI subtypes. Early recognition and reperfusion are critical. LAD occlusion may present with classic…
ECG Findings of LV Aneurysm
Key Points: Definition: A true LV aneurysm is a chronic, post transmural MI complication from scarred myocardium with akinetic or dyskinetic (paradoxical) wall motion. ECG hallmark: Persistent ST elevation in…
ST Elevation: DDx
Key Points: ST elevation describes an ECG finding, not a diagnosis. It reflects abnormal ventricular repolarization and can arise from ischemic, structural, metabolic, electrical, or extracardiac processes. Occlusion MI is…
Diffuse ST Elevation: DDx
Key Points: ST-segment elevation (STE) is an ECG finding, not a diagnosis. Multiple ischemic and non-ischemic processes can produce STE. Diffuse STE is often non-ischemic, in contrast to the regional…
Posterior STEMI: Criteria & Pitfalls
Key Points: High risk of missed diagnosis. Isolated posterior occlusion MI is frequently missed because ST elevation is absent on the standard 12-lead ECG. Instead, posterior infarction most often presents…
STEMI vs Early Repolarization: DDx
Key Points: Early repolarization (ER) is a common, benign ECG pattern that most often appears in young, healthy patients. It can closely resemble acute anterior STEMI, creating a high-risk diagnostic…
STEMI vs LV Aneurysm: DDx
Key Points: LV aneurysm pattern is a post MI scar pattern with persistent ST elevation in the prior infarct territory, usually with pathologic Q waves and a stable, non evolving…
ST Elevation in aVR with Diffuse ST Segment Depression: OMI Pattern
Key Points: Pattern, not a STEMI equivalent. ST elevation in aVR (≥1 mm), often with ST elevation in V1 and diffuse ST depression (≥1 mm in ≥6 leads), represents high-risk…
ST Elevation in aVR: DDx
Key Points: ST elevation (STE) in aVR with diffuse ST depression elsewhere most often reflects global subendocardial ischemia, not focal transmural infarction. High-risk coronary disease is one cause, not the…
ECG Tags
- A-Z
- ACS Mimics
- ACS-OMI
- Activation
- Advanced Level Curriculum
- Annual ECG Competition
- Anterior OMI
- Anterior STEMI
- Approach
- Arrest
- Arrhythmia
- Arrhythmogenic Cardiomyopathy
- Artifact
- ARVC
- ARVD
- Atrial Parasystole
- Attending
- AV Block
- aVF
- aVL
- aVR
- Axis
- Basics
- Board Review
- Bradyarrhythmia
- Chest Pain
- Clumped Beats
- Conduction
- Core
- Core Level Curriculum
- Critical ECG Patterns
- Curriculum
- DDx
- Delta
- Devices
- Diagonal Branch Occlusion
- Differential Diagnoses
- Diffuse ST Elevation
- Documentation
- Early Repolarization
- ECG Interpretation
- ECG Localization
- ECG Variant
- Education/Teaching
- Electrolytes
- Emergencies
- Emergent Cath Lab Activation
- EMS
- Expert Level Curriculum
- Foundations Level Curriculum
- Guidelines
- High-Lateral STEMI
- Hub
- Hyperacute T waves
- Hypercalcemia
- Hyperkalemia
- Hypermagnesemia
- Hypocalcemia
- Hypokalemia
- Hypomagnesemia
- Hyponatremia
- Hypothermia
- I
- II
- Index
- Inferior OMI
- Inferior STEMI
- Intervals
- Irregular
- Ischemia
- Ischemia & Infarction
- J Waves
- JT
- Juvenile T wave
- LAD Occlusion
- Lateral STEMI
- LBBB
- LCx Occlusion
- Lead Placement
- Life Savers
- LV an
- LV Aneurysm
- Mastery Level Curriculum
- Metabolic
- Mimics
- Morphology
- Narrow QRS
- Occlusion MI
- OMI Pattern
- Orthodromic AVRT
- Osborn Waves
- P Wave
- Paced Rhythms
- Pacemaker/ICD
- Paramedics
- Pauses
- PE
- Pediatrics
- Pericardial
- Pericarditis
- PGY-1
- PGY-2
- PGY-3
- PGY-4
- Post-Cardiac Arrest
- Posterior Extension
- Posterior MI
- Posterior STEMI
- PR
- Preexcitation
- Premature Complexes
- Prolonged QT
- Pulmonary Embolism
- Pulse-Tapping Artifact
- PVCs
- Q Wave
- QRS
- QT
- R Waves
- RAD
- Rate
- RBBB
- RCA Occlusion
- Regular
- Reperfusion
- Rhythm
- RR
- S Waves
- Segments
- Seizure
- Serial ECGs
- Sgarbossa
- Shock
- ST
- ST Depression
- ST Elevation
- STEMI
- STEMI Equivalent
- STEMI Mimics
- STEMI Negative OMI
- Stepwise
- Stroke
- Structural
- Students
- SVT
- Syncope
- T Wave Inversion
- T Waves
- Tachyarrhythmia
- Tachycardia
- Tamponade
- Terminal QRS Distortion
- Toxicology
- TP
- Traditional STEMI Criteria
- U Waves
- Unstable
- V1-V4
- V5
- V6
- Vectors
- Ventricular Repolarization
- Ventricular Rhythms
- Ventricular Tachycardia
- Voltage
- Waveforms
- Wide QRS
- Workflow
- WPW
© 2026 ECG Weekly. All rights reserved. | Terms of Use | Privacy Policy
Powered by the member(dev) platform
 Loading...
Loading...