Emergencies
Results:
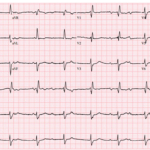
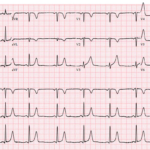
The Syncope ECG With Too Much P
A 68-year-old man has syncope, then has a second syncopal episode while lying still on a stretcher during evaluation at an outpatient clinic. He is sent emergently to the ED….

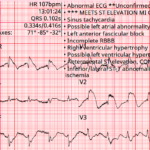
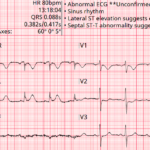
Modified Sgarbossa Criteria: STEMI Equivalent Pattern
Key Points: LBBB and ventricular-paced rhythms can hide acute coronary occlusion because abnormal depolarization creates expected secondary ST-T changes. Occlusion MI can still be recognized when those ST changes are…

Preexcitation Pitfalls (Part 4): Potpourri Cases & Final Teaching Points
A 49-year-old man arrives with palpitations and chest discomfort. The monitor shows an irregular, wide-complex tachycardia with varying morphology and rates nearing 250 to 300 bpm. The team debates polymorphic…
Preexcitation Syndromes: Overview
Key Points: Pre-excitation means an accessory pathway allows atrial impulses to reach the ventricle without traversing the AV node, producing early ventricular activation. A delta wave is the defining ECG…
Wolff-Parkinson White (WPW) Syndrome
Key Points: Pattern vs syndrome: WPW pattern is ECG evidence of pre-excitation without symptoms. WPW syndrome is pattern plus symptomatic tachyarrhythmia (palpitations, syncope, “seizure”, aborted sudden cardiac arrest). PR interval…
Atrial Flutter 1:1 Conduction
Key Points: Rare, high-risk rhythm. 1:1 flutter can drive ventricular rates into the 240–320 bpm range and can rapidly cause hypotension, ischemia, or collapse. It often mimics VT. Ask “how…
WPW Syndrome and Pseudo-MI Patterns
Key Points: WPW alters ventricular depolarization, producing secondary repolarization abnormalities that can mimic or mask myocardial infarction. ST-segment deviation in WPW is often non-ischemic, driven by abnormal activation via the…
Atrial Fibrillation with WPW (Pre-excited AF)
Key Points: Pre-excited AF is the most dangerous WPW rhythm. It can deteriorate quickly to VF because the accessory pathway may conduct atrial impulses to the ventricle at extreme rates….
WPW with Antidromic SVT (Antidromic AVRT)
Key Points: Antidromic AVRT is an AV re-entrant tachycardia that conducts antegrade down the accessory pathway and returns retrograde through the AV node (or another pathway), producing a regular wide-complex…
WPW with Orthodromic SVT (Orthodromic AVRT)
Key Points: Orthodromic AVRT is the most common tachyarrhythmia in WPW and presents as a regular narrow-complex SVT that is indistinguishable from AVNRT during the tachycardia. Mechanism: antegrade conduction down…
The Life Savers: Critical ECG Pattern Hub
Key Points: Critical ECG patterns represent time-sensitive, life-threatening cardiac or systemic conditions that demand immediate recognition to prevent death or irreversible organ injury. These are the “can’t-miss” ECGs. Use this…
Baltimore City EMS ECGs: Pitfalls and Mimics (Part 2)
A 54-year-old man presents to the emergency department by EMS with acute shortness of breath. A prehospital ECG triggers a STEMI alert based on the computer interpretation. The tracing shows…
Third-Degree AV Block (Complete Heart Block)
Key Points: Definition: Third-degree AV block is complete failure of conduction from atria to ventricles, resulting in independent atrial and ventricular activity—known as AV dissociation. Hallmark Feature: No P waves…
Second-Degree AV Block Type I (Mobitz I/Wenckebach)
Key Points: Definition: Progressive PR interval prolongation until one atrial impulse fails to conduct to the ventricles (P wave is non-conducted), after which the cycle repeats. Site of Block: Typically…
Second-Degree AV Block with 2:1 Conduction
Key Points: Definition: A form of second-degree AV block in which every other atrial impulse is blocked, producing a 2:1 atrioventricular conduction ratio. Typing Limitation: Differentiating between Mobitz I and…
High-Grade (Advanced) AV Block
Key Points: Definition: A severe form of second-degree AV block with two or more consecutive non‑conducted P waves (for example 3:1, 4:1). Do not force a Mobitz label when multiple…
Baltimore City EMS ECGs: Pitfalls and Mimics (Part 1)
A 68-year-old man is brought to the emergency department by EMS with acute chest discomfort. The following prehospital ECG was obtained and shows concave ST elevation across multiple leads. The…
Three More ECG Pitfalls That Punish Anchoring Bias
A 51-year-old man with lung cancer presents with shortness of breath and tachycardia. The arrival ECG shows an S1Q3 pattern and seems to support a familiar diagnosis that would normally…
Bidirectional Ventricular Tachycardia (BiVT)
Key Points: BiVT is a regular wide-complex tachycardia with strict beat-to-beat alternation of QRS axis and/or bundle-branch pattern (often an approximately 180° frontal-plane axis flip). In adults, assume digoxin toxicity…
Four ECG Pitfalls That Punish Anchoring Bias
A 43-year-old woman with sharp left-sided chest pain and minimal cardiac risk factors has an initial ECG that is not diagnostic for STEMI. She looks stable, but one feature on…
ECG Tags
- A-Z
- ACS Mimics
- ACS-OMI
- Activation
- Advanced Level Curriculum
- Annual ECG Competition
- Anterior OMI
- Anterior STEMI
- Approach
- Arrest
- Arrhythmia
- Arrhythmogenic Cardiomyopathy
- Artifact
- ARVC
- ARVD
- Atrial Parasystole
- Attending
- AV Block
- aVF
- aVL
- aVR
- Axis
- Basics
- Board Review
- Bradyarrhythmia
- Chest Pain
- Clumped Beats
- Conduction
- Core
- Core Level Curriculum
- Critical ECG Patterns
- Curriculum
- DDx
- Delta
- Devices
- Diagonal Branch Occlusion
- Differential Diagnoses
- Diffuse ST Elevation
- Documentation
- Early Repolarization
- ECG Interpretation
- ECG Localization
- ECG Variant
- Education/Teaching
- Electrolytes
- Emergencies
- Emergent Cath Lab Activation
- EMS
- Expert Level Curriculum
- Foundations Level Curriculum
- Guidelines
- High-Lateral STEMI
- Hub
- Hyperacute T waves
- Hypercalcemia
- Hyperkalemia
- Hypermagnesemia
- Hypocalcemia
- Hypokalemia
- Hypomagnesemia
- Hyponatremia
- Hypothermia
- I
- II
- Index
- Inferior OMI
- Inferior STEMI
- Intervals
- Irregular
- Ischemia
- Ischemia & Infarction
- J Waves
- JT
- Juvenile T wave
- LAD Occlusion
- Lateral STEMI
- LBBB
- LCx Occlusion
- Lead Placement
- Life Savers
- LV an
- LV Aneurysm
- Mastery Level Curriculum
- Metabolic
- Mimics
- Morphology
- Narrow QRS
- Occlusion MI
- OMI Pattern
- Orthodromic AVRT
- Osborn Waves
- P Wave
- Paced Rhythms
- Pacemaker/ICD
- Paramedics
- Pauses
- PE
- Pediatrics
- Pericardial
- Pericarditis
- PGY-1
- PGY-2
- PGY-3
- PGY-4
- Post-Cardiac Arrest
- Posterior Extension
- Posterior MI
- Posterior STEMI
- PR
- Preexcitation
- Premature Complexes
- Prolonged QT
- Pulmonary Embolism
- Pulse-Tapping Artifact
- PVCs
- Q Wave
- QRS
- QT
- R Waves
- RAD
- Rate
- RBBB
- RCA Occlusion
- Regular
- Reperfusion
- Rhythm
- RR
- S Waves
- Segments
- Seizure
- Serial ECGs
- Sgarbossa
- Shock
- ST
- ST Depression
- ST Elevation
- STEMI
- STEMI Equivalent
- STEMI Mimics
- STEMI Negative OMI
- Stepwise
- Stroke
- Structural
- Students
- SVT
- Syncope
- T Wave Inversion
- T Waves
- Tachyarrhythmia
- Tachycardia
- Tamponade
- Terminal QRS Distortion
- Toxicology
- TP
- Traditional STEMI Criteria
- U Waves
- Unstable
- V1-V4
- V5
- V6
- Vectors
- Ventricular Repolarization
- Ventricular Rhythms
- Ventricular Tachycardia
- Voltage
- Waveforms
- Wide QRS
- Workflow
- WPW
© 2026 ECG Weekly. All rights reserved. | Terms of Use | Privacy Policy
Powered by the member(dev) platform
 Loading...
Loading...